Welcome to The Mindful Motion Physical Therapist Specialist
2023-11-06
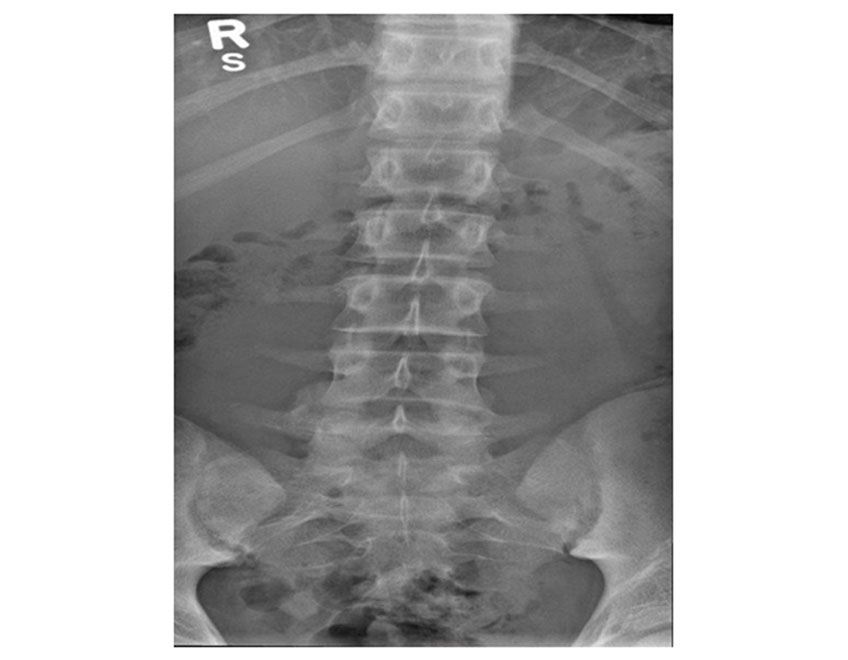
How many of you have been told that your X-ray looks like an 80-year-old? Or Have been told that your pain is due to disc bulge or meniscus injury? Guess what, new pain science suggests that pain is not related to the tissue injury or damage1. People can experience pain even when there is nothing wrong in their X-ray or MRI.
Pain is such a unique contextual experience which motivates us to do something about it. Pain signals human beings to take some action. Pain is an adaptive and protective mechanism that allows our body to heal. However, if pain protective mechanisms persist for longer duration, then it can hinder an individual's quality of life. So, what is pain? Is it helpful or harmful? And how is it defined?
The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential damage or described in terms of such damage”2.
Pain can be classified in many ways. One of the simplest ways to classify pain is based on duration:
Acute pain is sudden and generally short lasting. Majority of the time, the acute pain is correlated with some strain to tissue, organs, bones, and muscles. Brain perceives that there is danger or threat, and thus decides to generate pain. This prompts us to take some corrective action so that we can protect the body parts from further danger3. In this scenario, perception of pain is helpful because pain is motivating us to do something to dampen the danger or threat.
However, when pain persists beyond the initial injury, trauma or threat has subsided, then it is categorized as chronic pain. Generally, pain lasting beyond 6 months in duration is classified as chronic pain4. Chronic pain can significantly affect the quality of life and can lead to maladaptive unhealthy behavior.
Either pain is acute or chronic, the current pain science posits that pain is an output from the brain. I know it is hard to digest that brain is generating pain, right? Confused or may be your brain is overwhelmed because the above statement is challenging the belief about pain. No worries, you are not alone. So, let’s explore the current pain science, but it would be unfair not to know what is the ancient concept of pain science which is being practice by majority of healthcare providers.
Let us dive briefly into the history about pain science! No, I am not going to bore with you long historical dates.

Injury----> Pain travel through special fibers----->Brain. Descartes theory of pain5.
In 1664, Descartes, French philosopher, proposed that pain passes through a specialized nerve, which carries pain, and reaches some area in the brain and rings a bell to tell the brain about pain. His famous picture of man toes near the fire reverberates in many healthcare professional minds because that is the theory being practiced all along. Descartes, unarguably the most intelligent man of his time, was, in retrospect, got the theory of pain completely wrong as proved by current pain science research. Research in the last 40-50 years suggests that a flawed and inappropriate use of “tissue damage---nerve signals passing through the nerve---ringing bell in the brain” approach of treating persistent pain patients has been ineffective. Despite the new evidence about pain science, many of us practice the cartesian philosophy of finding structural problems or tissue problems as a reason for us to experience pain.
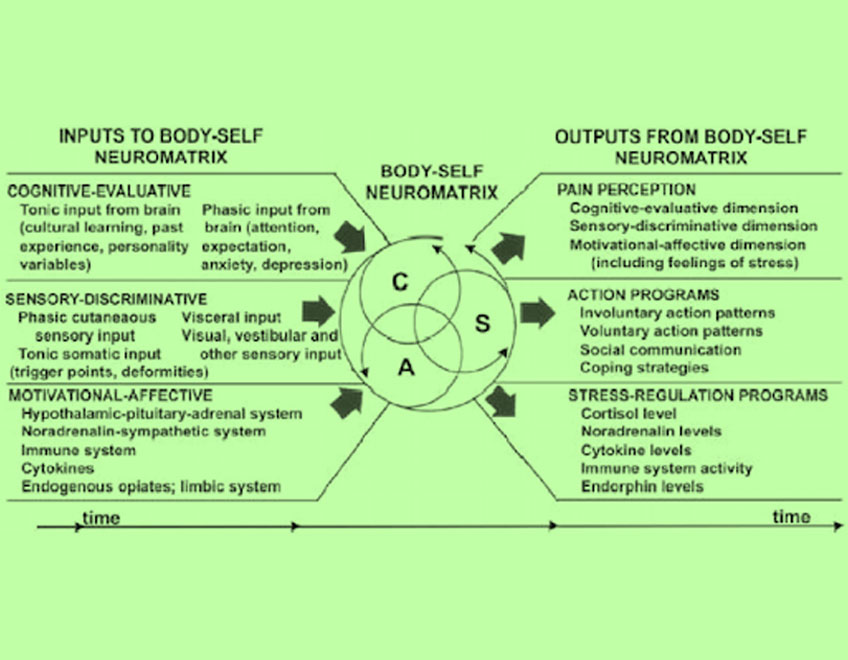
Due to continuous and incessant efforts of many scientists and researchers, like Ronald Melzack and Patrick Wall, we have better insight regarding pain science. Melzack’sNeuromatrix model changed the perspectives of understanding pain. The model suggests that that pain is an output from the brain due to complex neurological and neurochemical interaction of various input signals received from multiple sources. So, in simple terms this theory states that brain comes to a decision: is it worth being in pain at this moment, based on analysis form various signals it receives.
This new pain science theory completely threw out the notion that pain is related to bodily injury. Therefore, next time when you are experiencing pain or if you are a healthcare provider/ physical therapist treating patient with persistent pain, remember that structure abnormality or something wrong in your body is not the only reason for your pain. Or remind yourself “HURT IS NOT HARM”.
I know this might make you lightheaded or little dizzy, or your brain is wondering then how does a person experiences pain without tissue injury or pain signal? Well, we will discuss this new model, Melzack’sNeuromatrix, in next blog.
© all rights reserved: THE MINDFUL MOTION
Designed & Developed By: Vision Art Infotech